
How Do Peptides Work? Mechanisms Explained Simply
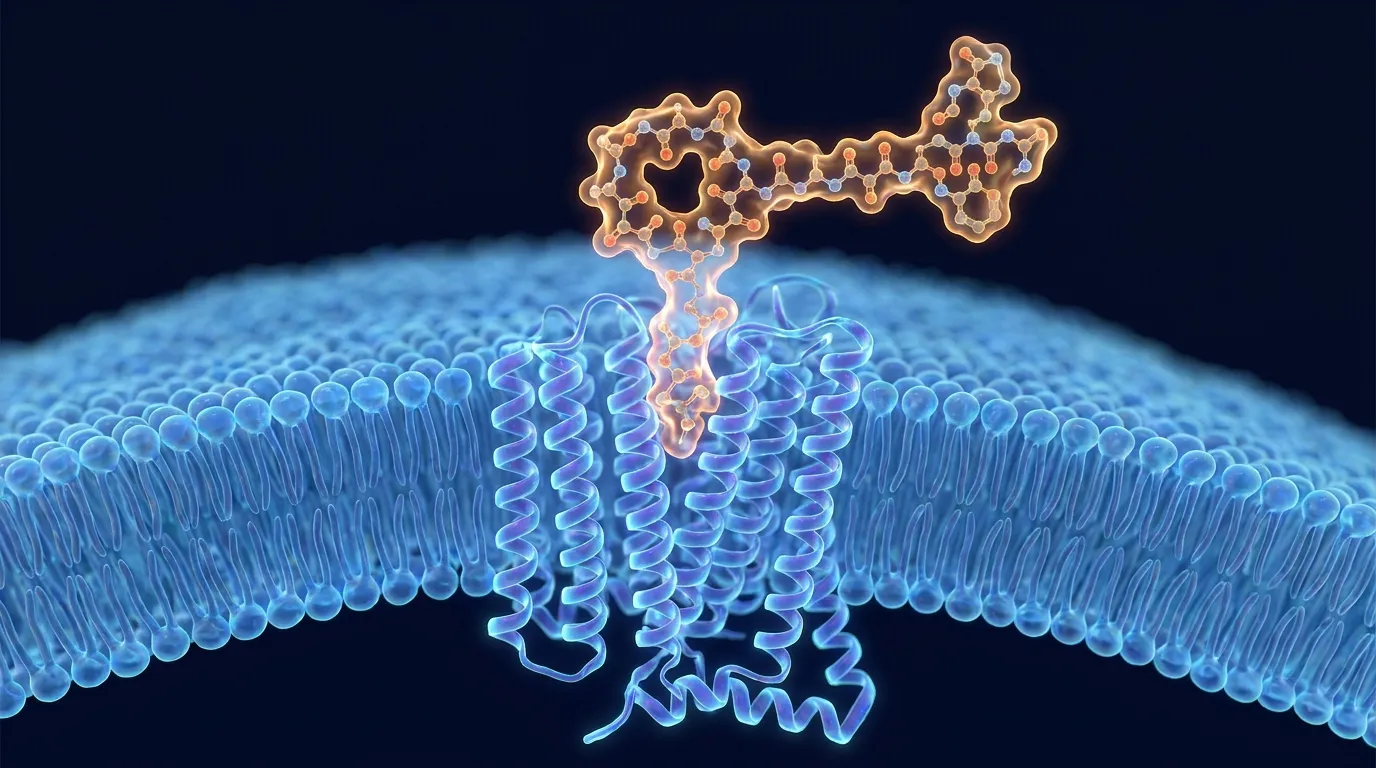
Peptides work mostly like keys: each one is a short chain of amino acids shaped to fit a specific "lock" called a receptor on the surface of a cell. When the peptide binds its matching receptor, it tells that cell to do something, such as release a hormone, take up sugar, or start repairing tissue. The peptide itself usually never enters the cell. It delivers a message at the door, and the cell's own machinery carries out the rest.
That single idea, a small molecule acting as a signal, explains almost everything about how peptides behave. It is why a tiny amount can have a large, specific effect; why most peptides are injected rather than swallowed; and why one peptide can do something completely different from another. This guide starts with the plain-English version and then goes into the real biochemistry: receptor binding, signal transduction, second messengers, agonists versus antagonists, and why peptides do not all act the same way. For the simpler question of what a peptide actually is, start with our peptide basics primer, and if any of the terms below trip you up, keep the plain-language glossary of peptide jargon open in a tab.
Key Takeaways
- Peptides act as chemical messengers. Most bind to a receptor on a cell's surface like a key in a lock, which switches a process on or off, rather than entering the cell themselves.
- The binding triggers a signaling cascade. A peptide hitting its receptor changes the receptor's shape, activates a relay (often a G protein), and produces "second messengers" inside the cell.
- A small signal becomes a big effect through amplification: one bound peptide can lead to thousands of downstream molecules, which is why micrograms can matter.
- Most peptides cannot cross the cell membrane because they are water-loving (hydrophilic), so they signal from outside. This also explains why many are injected, not swallowed.
- Agonists switch a receptor on; antagonists block it. This is the core of peptide pharmacology, and it is how drugs like GLP-1 agonists are designed.
- Peptides are short-lived by design. Enzymes break them down within minutes (native GLP-1 lasts about 2 minutes), so drug versions are engineered to resist that breakdown.
- Mechanism is not proof of benefit. A plausible mechanism does not mean a peptide is safe or effective in humans; many research peptides have little human evidence.
What does it actually mean for a peptide to "work"?
For a peptide to "work" means it delivers a signal that changes what a cell does, usually by binding to a receptor that recognizes its specific shape. A peptide is not a fuel and it is not a building block at this stage. It is a message.
Think of your body as a huge network of cells that need to coordinate. Peptides are one of the main ways cells talk to each other. Your body naturally makes thousands of signaling peptides, including many hormones, neurotransmitters, growth factors, and immune signals (NIH StatPearls, "Biochemistry, Peptide", 2023, retrieved 2026-06-15). Each one is built to be recognized by particular receptors, so the message lands only where it is meant to.
This is the difference between a peptide and, say, a vitamin or a sugar. A peptide's job is information, not energy or raw material. When people ask "how do peptides work," the honest one-line answer is: they bind a receptor and tell a cell what to do next. Everything below is the detail of how that happens.
Citation capsule. Peptides are short chains of amino acids that the body uses as signaling molecules, including hormones, neurotransmitters, and growth factors. Biologically active peptides "target specific proteins or protein-coupled receptors, such as G-protein-coupled-receptors (GPCRs)," and the resulting peptide-receptor complex "can then switch on or off a series of cascading reactions" that "control all cellular processing and functioning." Source: NIH StatPearls, "Biochemistry, Peptide," 2023.
How does a peptide bind to a cell? (The lock-and-key model)
A peptide works by fitting into a receptor that matches its exact shape, the way a key fits one lock, and that fit is what flips the switch. The peptide is the key; the receptor is the lock; the cell's response is the door opening.
Receptors are proteins that sit on (or in) cells and are built to recognize one signal. Because a peptide's shape comes from its specific amino acid sequence, only the right peptide fits the right receptor. A peptide with the wrong sequence will not fit, so it will not send the message. This is why the exact order of amino acids matters so much: change the sequence and you change the key.
Most peptide receptors sit on the outer surface of the cell. That is deliberate. Peptides are hydrophilic, meaning they dissolve in water but cannot slip through the cell's fatty membrane. "Receptors for most amino acid-derived hormones and all peptide hormones are located on the plasma membrane," in contrast to steroid hormones, which are fat-soluble and can pass right through the membrane to act inside the cell (The Medical Biochemistry Page, "Peptide Hormones and Their Receptors", 2023, retrieved 2026-06-15). So a peptide does its job at the doorstep, not inside the house.
When the key fits, the lock physically changes shape. That shape change on the inside of the cell is the actual "click" that starts the response. Nothing magical crosses the membrane; the receptor itself relays the message inward.
What happens after binding? (Signal transduction)
After a peptide binds, the receptor changes shape and hands the message off to molecules inside the cell, a relay process called signal transduction. The signal is converted from "a peptide is at the door" into "do this specific thing," step by step.
The most common relay system uses G protein-coupled receptors (GPCRs), the largest family of receptors in the human body. When a peptide binds a GPCR, the receptor's seven-part structure shifts, which activates an attached G protein on the inside of the membrane (Frontiers in Pharmacology, "Transmembrane signal transduction by peptide hormones via family B G protein-coupled receptors", 2015, retrieved 2026-06-15). For many peptide hormones, binding follows a neat two-part pattern: one end of the peptide grips the receptor's outer arm and the other end tucks into the membrane-spanning core, and that combined grip is what triggers the G protein (Frontiers in Pharmacology, 2015, retrieved 2026-06-15).
The activated G protein then turns on (or off) enzymes inside the cell, which generate small signaling molecules. Not every peptide uses a GPCR; some bind receptor tyrosine kinases (the route insulin uses) or ion channels. But across these systems the principle is identical: binding outside causes a change inside, and that change launches the next step.
The two-part grip, in plain terms
Many peptide hormones bind in two stages: first they latch onto the receptor's exposed outer region, then they slot into its core, and only the combined fit activates the signal. This is sometimes called the "two-domain" binding model.
The practical upshot is precision. A two-part grip means a receptor only fires when it sees a peptide that matches in two places at once, which keeps signaling specific and reduces accidental activation. Peptide hormones that work this way through family B GPCRs include GLP-1, glucagon, parathyroid hormone (PTH), secretin, and calcitonin, peptides ranging from roughly 26 to 114 amino acids long (Frontiers in Pharmacology, 2015, retrieved 2026-06-15).
How does a tiny peptide cause a big effect? (Second messengers and amplification)
A small amount of peptide produces a large effect because the signal is amplified: one bound peptide sets off a chain that creates thousands of "second messenger" molecules inside the cell. This is why peptides are dosed in micrograms or milligrams yet can shift whole body systems.
When a G protein is activated, it switches on enzymes that mass-produce small intracellular signals. "The main second messengers are cAMP, Ca2+, inositol-1,4,5-triphosphate (IP3 ... ), and diacylglycerol (DAG)" (The Medical Biochemistry Page, 2023, retrieved 2026-06-15). These molecules spread the message through the cell and switch on the machinery that produces the actual response, all the way down to changes in gene expression.
Which second messenger appears depends on which G protein the receptor uses:
| G protein type | What it does inside the cell | Typical second messenger |
|---|---|---|
| Gs | Activates adenylate cyclase | Raises cAMP |
| Gi | Inhibits adenylate cyclase | Lowers cAMP |
| Gq | Activates phospholipase C-beta | IP3 + DAG, releases Ca2+ |
The Gs route raising cAMP and the Gi route lowering it, with Gq producing IP3, DAG, and calcium, are the standard textbook couplings for peptide-hormone GPCRs (The Medical Biochemistry Page, 2023, retrieved 2026-06-15). The amplification at each step is the reason a faint signal at the surface becomes a loud instruction inside.

Agonist vs antagonist: turning the signal on or off
An agonist is a peptide that binds a receptor and switches it on; an antagonist binds the same receptor but blocks it, stopping the natural signal. This on/off distinction is the foundation of how peptide drugs are designed.
A natural peptide hormone is an agonist for its own receptor: it fits, it activates, the cell responds. A peptide drug can be built to do the same thing more strongly or for longer (an agonist), or to do the opposite, occupying the receptor so the body's own signal cannot get through (an antagonist). For disorders that involve peptide hormones, researchers deliberately design "agonist or antagonist ligands ... or inverse-agonist ligands" depending on whether they want to boost or block a pathway (Nature Reviews Drug Discovery, "Designing peptide receptor agonists and antagonists", 2002, retrieved 2026-06-15).
A competitive antagonist works by sitting in the same binding spot as the agonist, "in a manner that blocks the agonist from binding to the receptor site but does not bind in a manner that activates the transduction mechanism" (Nature Reviews Drug Discovery, 2002, retrieved 2026-06-15). In plain terms: the antagonist is a key that fits the lock but will not turn it, and while it is stuck in there, the real key cannot get in.
Our take: The most useful mental model for peptide pharmacology is the light switch. An agonist flips it on. An antagonist tapes it in place so it cannot move. The whole class of "GLP-1 agonist" weight-loss drugs is just a long-acting agonist that keeps the appetite-and-insulin switch pressed for far longer than the body's own version would.
Why are most peptides injected? (Stability and the digestion problem)
Most peptides are injected because if you swallow them, your digestive enzymes chop them apart before they can reach a receptor, and even in the blood, peptides are broken down within minutes. Their fragility is built into the chemistry.
Peptides are held together by peptide bonds, and your body is full of enzymes whose entire job is to cut those bonds. In the gut, protein-digesting enzymes treat a peptide like food. In the bloodstream, other enzymes called peptidases trim peptides down quickly. The clearest example is the natural hormone GLP-1: once secreted, it is "extremely susceptible" to the enzyme dipeptidyl peptidase-4 (DPP-4), giving active GLP-1 a half-life of only about 2 minutes (Wikipedia, "Glucagon-like peptide-1", 2026, retrieved 2026-06-15).
This is why peptide drugs are engineered for durability. By tweaking the sequence or attaching protective groups, chemists make versions that resist DPP-4 and other enzymes, turning a 2-minute natural signal into a drug that can be dosed once a day or once a week. The scale of that engineering gap is striking: semaglutide carries an elimination half-life of about 1 week (~165 hours) (FDA WEGOVY label, 2023, retrieved 2026-06-16), and tirzepatide about 5 days (FDA MOUNJARO label, 2022, retrieved 2026-06-16) — roughly a thousandfold longer than the native hormone they mimic. It is also why route of administration matters: subcutaneous injection skips the gut entirely, while oral peptide drugs are a hard and relatively new engineering achievement rather than the norm.

The practical side of administration, reconstitution, technique, and storage, is its own topic. We cover it in our peptide injections guide and the beginner roadmap in getting started with peptides. Here, the mechanism point is simple: peptides are short-lived messengers, and everything about how they are delivered works around that fact.
Do all peptides work the same way? (Mechanism families)
No. While most peptides act as receptor-binding messengers, they fall into a few mechanism families, and some work in less-defined ways. The shared logic is signaling; the specifics differ a lot.
Here are the main mechanism families people encounter, described by how they act rather than what they are marketed for:
- Hormone / metabolic signaling. Bind hormone receptors to regulate blood sugar, insulin, and appetite. GLP-1 drugs (semaglutide, tirzepatide) are agonists at the GLP-1 receptor, a family B GPCR (Frontiers in Pharmacology, 2015, retrieved 2026-06-15).
- Growth-hormone secretagogues. Rather than being growth hormone, these (sermorelin, ipamorelin, CJC-1295) bind receptors that tell the pituitary to release the body's own growth hormone, an indirect, upstream nudge.
- Tissue-repair signaling. Peptides studied for healing (BPC-157, TB-500) are proposed to influence repair and inflammation pathways, though their human evidence and exact receptors are far less established.
- Neuropeptides. Act as signals in the brain and nervous system, like oxytocin, binding neural receptors to affect mood, bonding, or pain.
- Antimicrobial peptides. A notable exception to the receptor model: many (such as LL-37, defensins) work physically, disrupting the membranes of bacteria rather than binding a single receptor.
The honest caveat is important here. For well-studied peptide medicines like GLP-1 drugs and insulin, the mechanism is mapped in detail. For many popular "research" peptides, the proposed mechanism is based on lab or animal work and a plausible signaling story, not confirmed human pharmacology. A clean diagram of a mechanism is not the same as proof that a compound is safe or effective in people.
How does the signal stop? (Signal termination)
The signal stops because the body actively shuts it off: receptors are desensitized and pulled inside the cell, second messengers are broken down, and the peptide itself is degraded by enzymes. Signaling is meant to be temporary, not permanent.
If a receptor stayed switched on forever, the cell could not respond to anything new. So within seconds to minutes of sustained signaling, GPCRs get tagged by enzymes (G protein-coupled receptor kinases), which recruit "arrestin" proteins that physically block the receptor from coupling to its G protein, a process called desensitization. Meanwhile the peptide is cleaved by peptidases and the second messengers are quickly degraded. The net effect is a built-in off-switch.
This matters for real-world use in two ways. First, it is why peptides are dosed repeatedly: the effect fades as the signal is cleared. Second, it is part of why some compounds are thought to lose effectiveness over time with continuous use, because chronic stimulation can keep receptors desensitized. The body is constantly resetting itself, which is exactly what a healthy signaling system should do.
Why does the same peptide do different things in different tissues?
The same peptide can have different effects in different parts of the body because the response depends on the cell, not just the signal. A peptide delivers an instruction, but each cell type interprets it through its own machinery.
Two factors drive this. First, not every cell carries the same receptors, so a peptide only acts where its receptor is present. Second, even cells that share a receptor can be wired to different downstream effects, so the identical signal produces one outcome in the gut and another in the brain. This "context matters" reality is why a single hormone can coordinate many organs at once, and why predicting a research peptide's full-body effect from one lab result is risky.
It is also a reason to be cautious about broad claims. A peptide marketed for one tissue may bind receptors elsewhere too, with effects that are not advertised. For anything you are evaluating, the relevant question is not only "what does this peptide do" but "where are its receptors, and what does each of those tissues do in response."
Peptides vs steroids vs small-molecule drugs: how the mechanism differs
Peptides differ from steroids and typical small-molecule drugs mainly in where and how they act: peptides signal from the cell surface with high specificity, steroids pass inside the cell, and small molecules can do either but are usually less selective. The mechanism shapes the whole profile.
A quick comparison of the core mechanism, not a safety or legality comparison:
| Feature | Peptides | Steroids | Small-molecule drugs |
|---|---|---|---|
| Where they act | Cell-surface receptors (mostly) | Inside the cell (intracellular receptors) | Inside or on the surface |
| Cross the membrane? | Usually no (hydrophilic) | Yes (fat-soluble) | Often yes |
| Specificity | Typically very high | Broad (affects many tissues) | Variable |
| Taken orally? | Usually no (digested) | Often yes | Usually yes |
| Lifespan in body | Short (minutes) unless engineered | Longer | Variable |
Peptides' high specificity and tendency toward lower off-target toxicity are exactly why they are an attractive drug class, qualities highlighted in reviews of therapeutic peptides (Nature, Signal Transduction and Targeted Therapy, "Therapeutic peptides: current applications and future directions", 2022, retrieved 2026-06-15). The trade-off is fragility and the need for injection. We keep the steroid comparison at the mechanism level here; the chemical-class and legal differences are covered in our glossary and legality guide.
A short walk-through: how a GLP-1 peptide works, step by step
To make the mechanism concrete, here is how a GLP-1 peptide produces its effect, from injection to outcome. GLP-1 is the clearest example because it is well-studied and behind today's best-known peptide drugs.
- Delivery. The peptide is injected under the skin, bypassing the digestive enzymes that would destroy it if swallowed.
- Binding. It travels to target cells and binds the GLP-1 receptor, a family B GPCR, gripping it in the two-part pattern that activates it (Frontiers in Pharmacology, 2015, retrieved 2026-06-15).
- Relay. The activated receptor switches on a Gs protein, which turns on adenylate cyclase and raises cAMP inside the cell (The Medical Biochemistry Page, 2023, retrieved 2026-06-15).
- Response. In pancreatic beta cells, that signal promotes insulin secretion in a glucose-dependent way, the hallmark effect of GLP-1 (Wikipedia, "Glucagon-like peptide-1", 2026, retrieved 2026-06-15). Elsewhere it slows stomach emptying and reduces appetite.
- Durability by design. Native GLP-1 would be gone in about 2 minutes via DPP-4, so drug versions are engineered to resist that enzyme and last far longer (Wikipedia, 2026, retrieved 2026-06-15).
That sequence, deliver, bind, relay, respond, persist, is the whole mechanism story in one example. Different peptides swap in different receptors and outcomes, but the skeleton is the same.
Frequently Asked Questions
The bottom line
Peptides work by carrying messages, not by acting as fuel or building blocks. Each one is a short amino acid chain shaped to fit a specific receptor, and when it binds, it changes that receptor's shape and triggers a signaling cascade inside the cell. A small signal at the surface is amplified into a large, specific effect, which is why micrograms can matter. Agonists switch the receptor on; antagonists block it; and the whole signal is short-lived because enzymes clear peptides within minutes.
If you remember one thing, make it the lock-and-key picture: the peptide is the key, the receptor is the lock, and the cell's own machinery is what actually does the work once the door opens. That model makes sense of nearly every peptide question, from why most are injected to why the same compound can do different things in different tissues. Just keep the honest caveat in view: a clear mechanism is a starting point, not proof of benefit or safety. For the basics of what peptides are, see what are peptides; for the practical side, see getting started with peptides; and for anything you might consider using, talk to a qualified healthcare professional first.
Sources
- NIH / StatPearls (Forbes J, Krishnamurthy K). "Biochemistry, Peptide." StatPearls Publishing, 2023. Retrieved 2026-06-15. https://www.ncbi.nlm.nih.gov/books/NBK562260/
- Culhane KJ, et al. "Transmembrane signal transduction by peptide hormones via family B G protein-coupled receptors." Frontiers in Pharmacology, 2015 (PMC4633518). Retrieved 2026-06-15. https://pmc.ncbi.nlm.nih.gov/articles/PMC4633518/
- The Medical Biochemistry Page. "Peptide Hormones and Their Receptors." 2023. Retrieved 2026-06-15. https://themedicalbiochemistrypage.org/peptide-hormones-and-their-receptors/
- Hruby VJ. "Designing peptide receptor agonists and antagonists." Nature Reviews Drug Discovery, 2002 (PubMed 12415245). Retrieved 2026-06-15. https://pubmed.ncbi.nlm.nih.gov/12415245/
- Wikipedia. "Glucagon-like peptide-1." Retrieved 2026-06-15. https://en.wikipedia.org/wiki/Glucagon-like_peptide-1
- U.S. Food and Drug Administration. "WEGOVY (semaglutide) injection — Prescribing Information." 2023. Retrieved 2026-06-16. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/215256s007lbl.pdf
- U.S. Food and Drug Administration. "MOUNJARO (tirzepatide) injection — Prescribing Information." 2022. Retrieved 2026-06-16. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/215866s000lbl.pdf
- Wang L, Wang N, Zhang W, et al. "Therapeutic peptides: current applications and future directions." Signal Transduction and Targeted Therapy (Nature), 2022. Retrieved 2026-06-15. https://www.nature.com/articles/s41392-022-00904-4
- Wikipedia. "Peptide." Retrieved 2026-06-15. https://en.wikipedia.org/wiki/Peptide